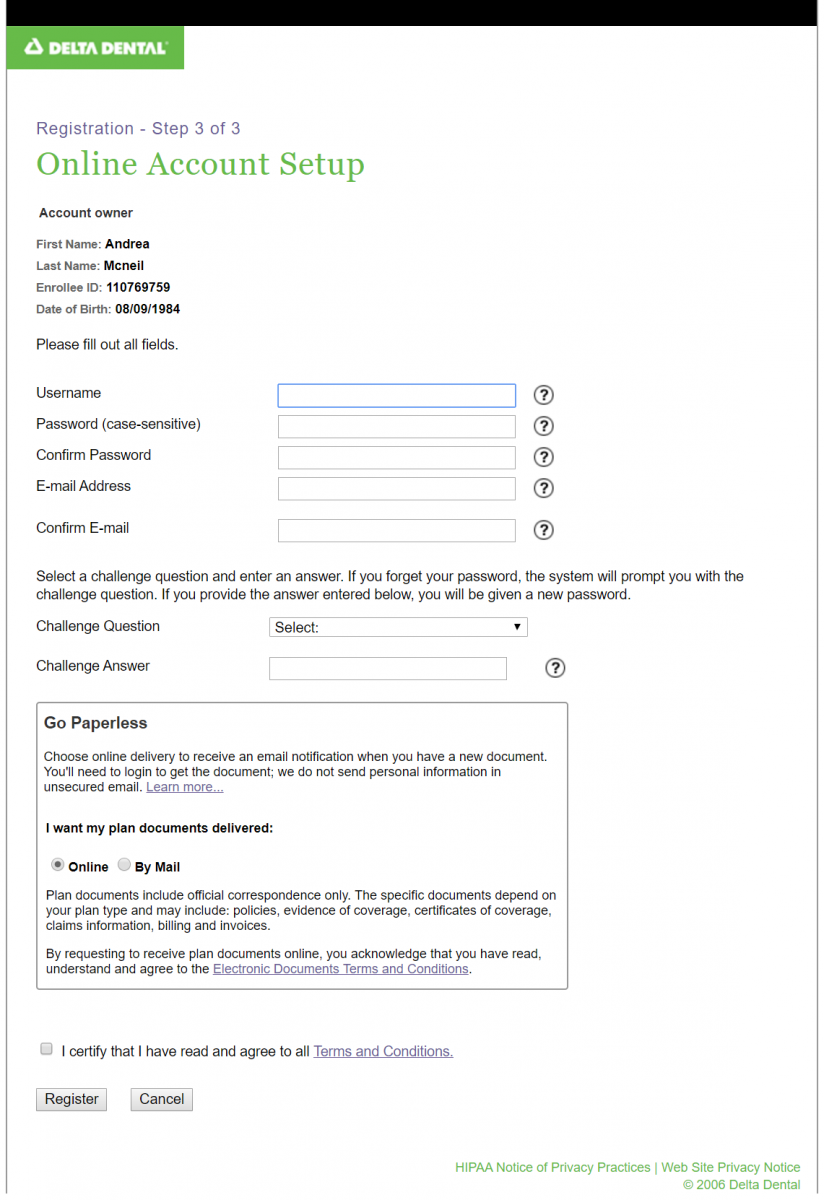
delta dental application form
Locum tenens provider form. ENROLLMENTCHANGE FORM - NY Delta Dental of New York Inc.
Dental Insurance
Appeal Form - Information on how to appeal your claim.

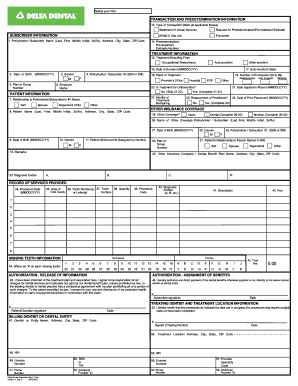
. Use this form to file a claim for services performed in the United States. Theres no hassle in working through claims saving you time and frustration. STAPLE X-RAYS TO FORM FORM DDNY-0016-04-10 EMPLOYEE MUST COMPLETE ITEMS 1 THROUGH 15 LAST FIRST ZIP CODE 6.
With Delta Dental we keep you smiling. Dentist Administrative Forms and Resources. To access a dental claim form enrollees can log into Member Portal.
Easily download and submit the form or application that relates to your needs. More Americans choose Delta Dental than any other dental insurance provider. Delta Dental PPO participation packet request.
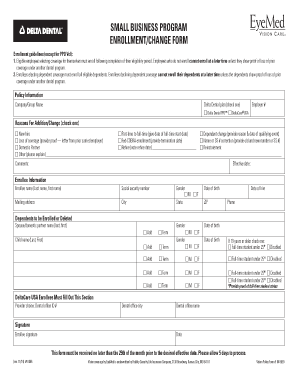
Join our dentist network. Small Business Program. Download Insurance Forms Information.
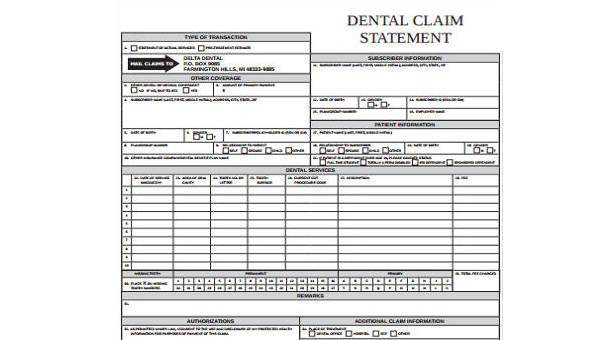
Name of Other Dental Carrier Policy Holder Name firstlast Date of Birth Effective Date of. Use this form to view overage dependents information or if youre having custody issues. Our mission is to improve lives by promoting optimal oral health.
Adults and parents of children ages 12 and younger illuminate what they thought about their oral health and what. Please mail your claim form to. EMPLOYER COMPANY NAME AND ADDRESS.
Little Rock AR 72231. They can also call Customer Service at 877 395-9420 or send an email to. Arizona Dental Insurance Service Inc.
Find solutions that make it easier to manage your practice like benefit information and claims status. Get the most out of your companys Delta Dental benefits. We would like to show you a description here but the site wont allow us.
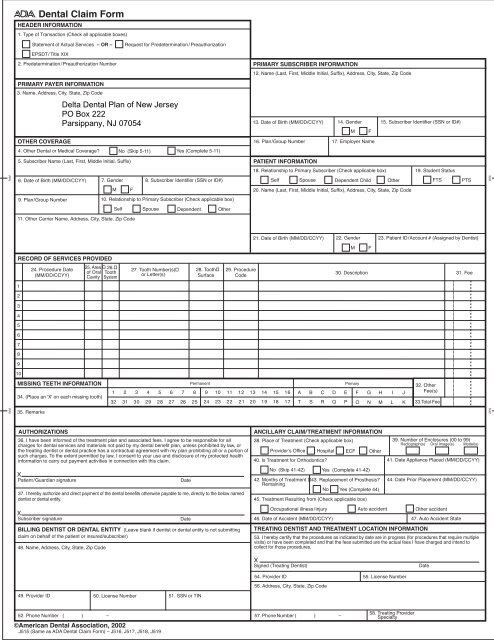
Delta Dental of Arizona is a part of Delta Dental Plans. Delta Dental of New Jersey. Dba Delta Dental of Arizona.
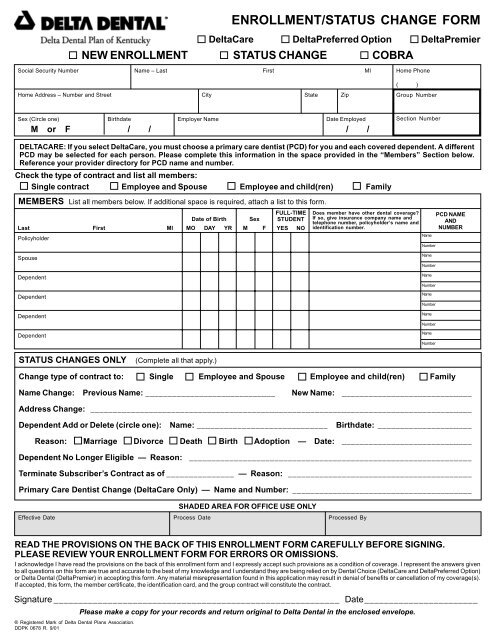
EMPLOYER COMPANY NAME AND ADDRESS. Authorization Agreement for Automatic Payments. For your own information and protection certain facts should be pointed out to you which could affect your.
STAPLE X-RAYS TO FORM-0016-04-10 EMPLOYEE MUST COMPLETE ITEMS 1 THROUGH 15 LAST FIRST ZIP CODE 6. MNND Eligibility EnrollmentUpdate Form. This will allow Delta Dental of Washington to release relevant information to the chosen party.
Whether youd like to modify your current plan or apply for new benefits youll find the. Findings from the Delta Dental-commissioned research of 2000 US. Issued by Delta Dental you must sign and return this form with your application.
Direct Debit Authorization ACH Form. Thats why most dentists choose to work with Delta Dental to protect their patients. MN Membership Enrollment Form Spanish Small Group Pooled MN ND Enrollment Form for.

Delta Dental Enrollment Form
Delta Dental Enrollment Form

Delta Dental Enrollment Form Fill Online Printable Fillable Blank Pdffiller
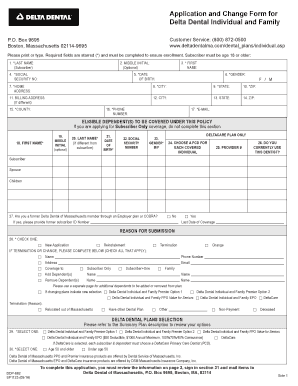
Fillable Online Enrollment Form Delta Dental Of Massachusetts Fax Email Print Pdffiller

Getting Started With Your Dental Benefits Delta Dental Mass
Delta Dental Of Washington Dental Insurance Delta Dental Of Washington

Dental Claim Submission Form Fill Out Sign Online Dochub
Delta Dental Enrollment Form California Fill Out And Sign Printable Pdf Template Signnow
Delta Dental Claim Form Fill Out And Sign Printable Pdf Template Signnow
Dental Illinois Institute Of Technology
Free 8 Dental Claim Forms Samples In Ms Word Pdf
![]()
Delta Dental For Dentists Delta Dental

Delta Dental New Patients Rubal Dentistry
Delta Dental Claim Form

Delta Dental Dental Insurance Dr Robert A Whitmore
Dental Insurance

Delta Dental 101
Delta Dental Group Spanish Healthcare Reform Certified Hcr Plans Membership Enrollment Form Fill And Sign Printable Template Online
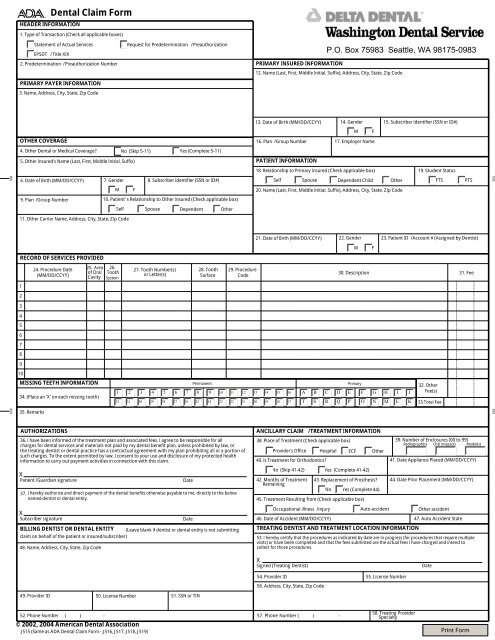
Delta Dental Claim Form Washington Dental Service